안녕하세요 창원 함소아 한의원입니다 ^^ 오늘은 축농증에 대해서 알아보겠습니다.축농증이란?

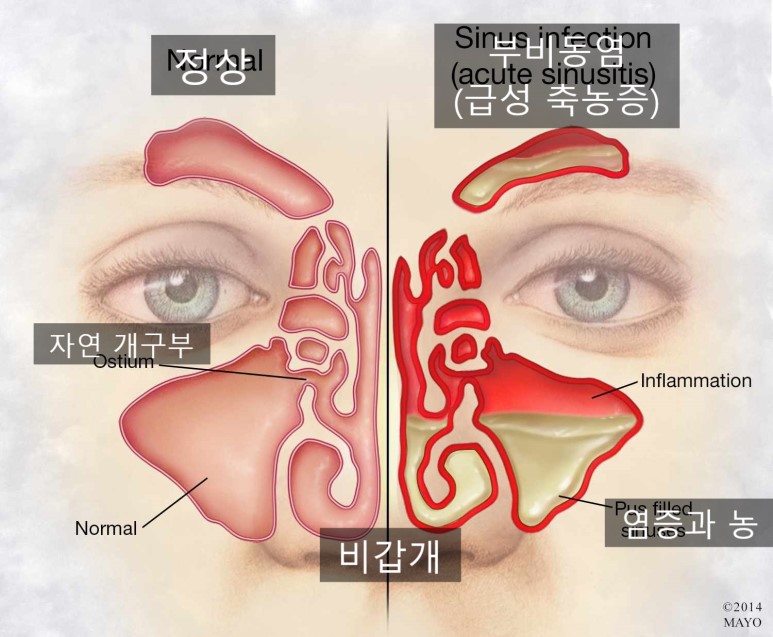
축농증과 부비동염은 같은 질환입니다. 코와 연결되어 있는 동굴 형태의 공간인 부비동에 고름이 쌓이는 질환입니다. 감기 후 콧물, 코막힘 등의 코의 증상이 길어지거나 알레르기성 비염이 심한 경우에는 위의 그림의 갈고리 모양의 비등견이라는 구조물의 점막이 붓습니다. 부은 점막에서는 콧물이 분비되어 콧속을 채워줍니다.
그로 인해 코와 연결되어 있는 부비강의 자연 개구부가 막혀 점막에서 배출되는 콧물과 염증이 쌓여 축농증이 됩니다. 이와 같이 축농증은 주로 감기나 비염의 합병증으로 많이 나타납니다. 감기가 바이러스에 의해 유발되기 때문에 축농증도 세균성보다 바이러스성인 경우가 더 많습니다. 그래서 항생제가 필요하지 않은 경우도 많다고 해요. 대부분의 경우 축농증으로 심각한 합병증이 발생하지 않고 완치할 수 있는 질환입니다.축농증의 진단 과거에는 진단을 위해 X선이나 CT 등의 영상 검사를 실시하고 있었지만 지금은 더 이상 권고되지 않습니다.< 미국 소아과 학회 축농증 진료지침 2013>OBJECTIVE: To update the American Academy of Pediatrics clinical practice guideline regarding the diagnosis and management of acute bacterial sinusitis in children and adolescents. METHODS: Analysis of the medical literature published since the last version of the guideline (2001). RESULTS: The diag…pediatrics.aappublications.orgKey Action Statement 2 AClinicians should not obtain imaging studies ( plain films , contrast – enhanced computed tomography [ CT ] , MRI , or ultrasonography ) to distinguish acute bacterial sinusitis from viral URI ( Evidence Quality : B ; Strong Recommendation ) .
KAS Profile 2AThe purpose of this key action statement is to discourage the practitioner from obtaining imaging studies in children with uncomplicated acute bacterial sinusitis. As emphasized in Key Action Statement 1, acute bacterial sinusitis in children is a diagnosis that is made on the basis of stringent clinical criteria that describe signs, symptoms, and temporal patterns of a URI. Although historically imaging has been used as a confirmatory or diagnostic modality in children suspected to have acute bacterial sinusitis , it is no longer recommended .
The membranes that line the nose are continuous with the membranes (mucosa) that line the sinus cavities, the middle ear, the nasopharynx, and the oropharynx. When an individual experiences a viral URI, there is inflammation of the nasal mucosa and, often, the mucosa of the middle ear and paranasal sinuses as well. The continuity of the mucosa of the upper respiratory tract is responsible for the controversy regarding the usefulness of images of the paranasal sinuses in contributing to a diagnosis of acute bacterial sinusitis .
As early as the 1940s, observations were made regarding the frequency of abnormal sinus radiographs in healthy children without signs or symptoms of current respiratory disease.19 In addition, several investigators in the 1970s and 1980s observed that children with uncomplicated viral URI had frequent abnormalities of the paranasal sinuses on plain radiographs.20–22 These abnormalities were the same as those considered to be diagnostic of acute bacterial sinusitis ( diffuse opacification , mucosal swelling of at least 4 mm , or an air – fluid level ) . 16
As technology advanced and CT scanning of the central nervous system and skull became prevalent, several studies reported on incidental abnormalities of the paranasal sinuses that were observed in children.23,24 Gwaltney et al25 showed striking abnormalities (including air-fluid levels) in sinus CT scans of young adults with uncomplicated colds. Manning et al26 evaluated children undergoing either CT or MRI of the head for indications other than respiratory complaints or suspected sinusitis. Each patient underwent rhinoscopy and otoscopy before imaging and each patient’s parent was asked to fill out a questionnaire regarding recent symptoms of URI. Sixty-two percent of patients overall had physical findings or history consistent with an upper respiratory inflammatory process, and 55% of the total group showed some abnormalities on sinus imaging ; 33 % showed pronounced mucosal thickening or an air – fluid level . Gordts et al27 made similar observations in children undergoing MRI . Finally , Kristo et al28 performed MRI in children with URIs and confirmed the high frequency ( 68 % ) of major abnormalities seen in the paranasal sinuses .
In summary, when the paranasal sinuses are imaged, either with plain radiographs, contrast-enhanced CT, or MRI in children with uncomplicated URI, the majority of studies will be significantly abnormal with the same kind of findings that are associated with bacterial infection of the sinuses. Accordingly, although normal radiographs or CT or MRI results can ensure that a patient with respiratory symptoms does not have acute bacterial sinusitis, an abnormal image cannot confirm the diagnosis. Therefore, it is not necessary to perform imaging in children with uncomplicated episodes of clinical sinusitis. Similarly, the high likelihood of an abnormal imaging result in a child with an uncomplicated URI indicates that radiographic studies not be performed in an attempt to eliminate the diagnosis of sinusitis.
이미 1940년대에 호흡기 증상이 없는 건강한 아동에서도 부비강 X선 사진이 축농증 소견으로 자주 나타난다는 점이 관찰됐고 1970년대80년대에도 감기 아동에게서 X선 이상 축농증 소견이 자주 관찰된 바 있다.
감기에 걸리지 않은 젊은 성인에서도 CT상에서 현저한 축농증 소견이 나타난다는 연구결과와 일반 감기임에도 68%는 MRI 상축농증 소견을 보인다는 연구결과가 있다.
따라서 영상검사상 부비강 정상소견은 부비강 세균 감염이 없는 것은 확인되지만 영상에서 비정상적으로 나타나더라도 세균 감염을 확인할 수 있다.
축농증 비내경 소견
감기 환자가 콧물이나 기침이 10일 이상 지나도 호전되지 않거나 더 악화될 경우 고열과 노란 콧물이 3일 이상 지속되면 축농증으로 진단할 수 있습니다.축농증 증상<화농성 콧물, 코막힘>축농증에 시달리는 어린이는 보통 노랗거나 녹색의 화농성 콧물을 보이기도 합니다. 축농증 때문에 콧물을 계속 흘리는 아이도 있지만 코가 안쪽에만 차서 콧물이 보이지 않는 아이도 있어요
<후비루·기침>축농증으로 코 안쪽이 막혀 콧물이 뒤로 흘러내릴 수 있습니다. 따라서 뒷목에서 후비루를 보이거나 뒷목이 가렵고 기침을 하는 경우가 많습니다.
<피로, 발열> 축농증으로 고열이 나는 경우는 많지 않지만 급성 축농증 초기에는 발열 증상이 나타날 수도 있습니다. 또한 축농증 때문에 콧속의 환기가 올바르지 않으면 만성피로와 같은 증상도 나오게 됩니다.
<안면통, 두통> 코와 연결된 부비동으로 통하는 구멍이 막혀 부비강에 고름이 쌓이면 광대뼈, 이마, 눈 안쪽 등 다양한 부위에 두통과 같은 통증이 생깁니다. 그래서 아이가 안면통이나 두통을 호소할 수 있어요.축농증 치료 축농증은 소아과에서도 치료 기간이 길게 볼 수 있는 질환 중 하나입니다. 만성의 경우 8주를 기본으로 하여 항생제 치료를 하게 됩니다. 항생제는 아이들의 소화기에 무리를 줘 장기적으로 면역력을 떨어뜨리는 원인이 되기 때문에 꼭 필요한 경우에만 사용하는 것이 중요합니다.
부비강 기능을 유지하기 위해서는 점막 섬모 운동을 회복시키는 것이 중요합니다. 창원 함소아에서는 면역력 강화와 어린이의 체질적 취약점 개선에 초점을 맞추고, 부종을 완화하여 농 배출을 돕도록 치료합니다.
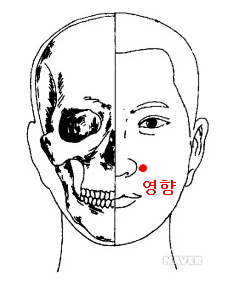
또한 침, 뜸, 호흡기 치료, 코에 뿌려 바르는 한방 외용제를 이용한 치료도 함께 실시합니다. 침이나 뜸의 치료는 코의 기혈 순환을 깨끗하게 하고 코 점막을 튼튼하게 합니다.축농증(부비강염 생활관리 1) 코막힘 완화에 좋은 경혈을 자주 마사지 하십시오.

코 양쪽 콧방울 바로 옆에 움푹 들어간 곳(영향 구멍)을 집게손가락으로 꾹꾹 아픈 느낌이 들 정도로 마사지해 주세요 코 안의 염증이 가라앉아 코 점막이 건강해지는 데 도움이 됩니다.
미지근한 물을 자주 마시게 해주세요.
축농증으로 콧물이 목에 걸리면 아이가 기침을 자주 하게 됩니다. 이때 미지근한 물을 자주 먹이면 목 주위의 점막이 촉촉해지고 코의 가래 등이 풀어지면서 증상을 완화시킵니다.
3) 평소 냉난방기 사용을 최소화하십시오.

히터, 에어컨과 같은 냉난방기는 실내 공기를 바로 건조시키고 바람 자체도 코에 좋지 않은 영향을 줍니다. 겨울철 난방을 시작한 경우에는 반드시 가습도 함께 가져와 주시기 바랍니다. 실내온도 22~23도, 습도는 55% 정도를 유지합니다.
자, 지금까지 축농증에 대해 알아보았습니다. 우리 아이의 건강을 기원합니다.